The American firearms industry has quietly built its training culture, its product design, and its service standards around a shooter who represents a shrinking share of its actual customer base. The result is a profession that is technically sophisticated and practically inadequate for the clients it will serve over the next two decades. Seth Cohen, gunsmith and firearms instructor, presents the Adaptive Protocol -- a structured, defensible, and immediately deployable methodology for closing that gap.
THE INDUSTRY HAS THE WRONG SHOOTER IN MIND
Most mainstream firearms training curricula still assume a shooter who is physically capable, mid-career, and in possession of the grip strength, visual acuity, and joint mobility that contemporary instruction was designed around. The drills, the draw standards, the magazine protocols, the slide manipulation techniques – nearly all of which were optimized for that person.
That person is a diminishing fraction of the actual shooter population. And the profession has not caught up.
The Baby Boomer generation represents the largest, most experienced, and most financially committed cohort of gun owners in American history. According to National Shooting Sports Foundation data, first-time buyers skew younger, but sustained ownership, carry frequency, and training investment all index highest in shooters over fifty. The Centers for Disease Control reports that nearly half of Americans over sixty-five are managing some form of diagnosed arthritis -- a condition that directly affects grip strength, trigger control, the ability to manipulate a modern semi-automatic firearm and not mentioning that the pain these conditions cause robs one of the ability to focus and enjoy the activities that had been enjoyed in the past. These are not clients on the fringes of the population; they are the core of the training market, and most current practice has no structured answer for what they need.
The industry's response has been inadequate. Larger controls on a handful of models. Reduced-recoil ammunition is marketed as a concession to few. No intake standards or structured assessment methodology. No professional consensus on what constitutes defensible work on a carry firearm destined for hands that may tremble and lose strength to manipulate controls designed for people in their prime. Practitioners who have not built adaptive competence are not neutral. They are already behind the clients standing in front of them.
What is missing is not compassion. Most instructors and gunsmiths genuinely care about their older clients. What is missing is a framework -- and every day without one is another client who walks away believing there is nothing left to be done.
Most practitioners care about their older clients. What is missing is a framework.
WHAT CURRENT PRACTICE IS GETTING WRONG
The failures in current professional practice are not failures of intent. They are failures of structure. Without a defined methodology, gunsmiths and instructors default to familiar tools applied in an intuitive order rather than a defensible one.
What the industry currently calls custom work is often improvisation without diagnosis. A trigger job performed without intake. A slide aid is sold without observing why the shooter is failing. A platform recommendation made based on preference rather than assessment. The table below names the five most common failure patterns and their direct consequences for aging clients.
| CURRENT PRACTICE FAILURE | CONSEQUENCE FOR THE AGING SHOOTER |
|---|---|
| Trigger job as the default intervention | Modifies a safety-critical component without addressing the shooter's actual physical limitation. Creates liability without solving the problem. |
| No structured intake or diagnostic observation | Interventions are guesses rather than conclusions. The wrong modification is applied with confidence, and its failure is attributed to the shooter. |
| Gear substituted for diagnosis | Appliances are sold rather than prescribed. The shooter accumulates equipment that may or may not address their specific failure point. |
| No documentation standard | No professional record exists. If a modified carry firearm is used in a defensive incident, the practitioner has no defensible account of their decisions. |
| Binary outcome framing | Shooters are told they can either perform as they always have or stop shooting. The adaptive middle ground is never offered, and experienced shooters exit the sport. |
The most consequential failure is the last one. The binary framing -- perform as you always have or stop shooting -- is quitting dressed as pragmatism. Experienced shooters told there is nothing to be done exit the sport quietly, surrender carry permits, and lose a measure of independence they have carried for decades. That outcome is very preventable.
The Adaptive Protocol is the structured answer the profession has been missing. It requires no new technology, no specialized equipment, and no credentials beyond what a competent instructor or gunsmith already holds. It requires a change in the order of operations -- and the discipline to follow that order every time.
Adaptive work begins with diagnosis, not modification.
WHERE THIS FRAMEWORK CAME FROM
I did not develop this protocol in a classroom. I developed it by watching people I respect manage pain they did not talk about. Instructors whose names appear on training DVDs and magazines would finish a long demonstration, step off the line, and quietly flex a stiff hand or roll a sore shoulder when they thought no one was watching. Their technique was still sound, fast, and certain. The arthritis was hidden inside it. That observation planted a question that stayed with me: if experienced instructors absorb this cost invisibly, what happens to the sixty-five-year-old student who has no technique or no technique left to hide behind?
When I began teaching senior-dominant classes in Central Florida, the question became concrete. I watched students squint at front sights that no longer resolved. I watched them wrestle with slides and magazines that younger hands took for granted. The determination was intact, but the fear was also intact. Fear of dropping the gun. Fear of failing to rack or being unable to rack the slide under stress. Fear of having to give up carrying, and what that meant for their independence, for their capability, and for the people they were committed to protecting.
One afternoon, a student stopped mid-drill, set the gun down on the bench, and said quietly: I think I am done. Not frustrated or angry. Just done. She had made her peace with it on the drive over and came to class to confirm what she had already decided. That moment is the reason this framework exists. She was not done. She needed a loader, a grip adjustment, and someone who knew the difference between a strength problem and a technique problem. She was back the following week…loving it.
My model for what adaptation actually looks like came from my father, who had been blind since he was eighteen. My image of competence was never a man defined by limitation. It was a man who found ways to do nearly everything differently, supported by organizations that built solutions for his actual capabilities rather than demanding he perform for a standard designed for someone else. That is the root of this framework. Adaptation is not accommodation in the diminishing sense. It is professional recognition that the person in front of you deserves a solution built for who they are, not for who the catalog picture assumes they should be.
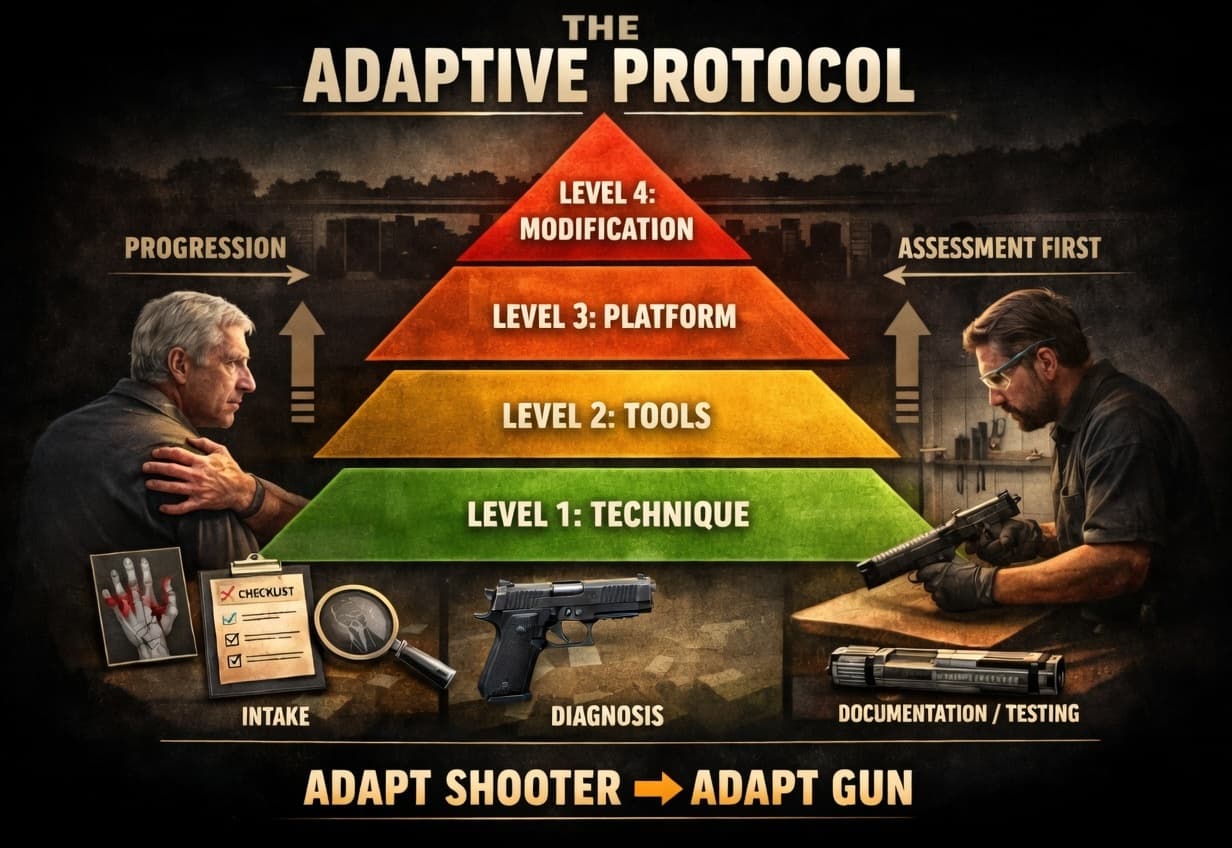
THE ADAPTIVE PROTOCOL: HIERARCHY OF INTERVENTION
The Adaptive Protocol is a structured decision-making sequence governing how a practitioner approaches a shooter whose physical capabilities have changed. Its organizing principle is least invasive first: exhaust every option at each level before advancing to the next. Advancement is governed by clinical observation, not by what is fastest or most billable. The protocol proceeds through four levels, and the threshold for advancing is demonstrable insufficiency at the current level.
| THE ADAPTIVE PROTOCOL | HIERARCHY OF INTERVENTION | ||
|---|---|---|
| LEVEL 1 Technique & Posture |
Adapt grip, stance, presentation, trigger mechanics, and reload procedure to current physical capability. Touch nothing. | ▼ Advance only if: complaint persists after full technique revision |
| LEVEL 2 Appliances & Externals |
Introduce loaders, rackers, grip aids, optics, and carry reconfiguration. The gun stays stock. | ▼ Advance only if: appliances are insufficient or unavailable for the specific need |
| LEVEL 3 Platform & Caliber |
Select a firearm matched to current strength, dexterity, and visual acuity. Reversible. The shooter retains options. | ▼ Advance only if: platform change is not feasible or remains insufficient |
| LEVEL 4 Internal Modification |
Springs, triggers, controls, integral cocking aids -- only after Levels 1 through 3 are fully exhausted and documented. Gun is opened in Level 4. | |
LEVEL 1: TECHNIQUE AND POSTURE
The first question is always whether the presenting problem is a technique problem. Grip, stance, presentation mechanics, trigger discipline, and reload procedures can all be adapted to the current physical reality without touching the firearm or introducing any appliance. A shooter whose arthritis has altered their natural grip may need a fundamentally different hand position. A shooter managing a knee replacement may need a redistributed stance. These interventions cost nothing, leave the platform unaltered, and resolve a substantial portion of presenting complaints when applied with precision. Most instructors underestimate what is achievable at Level 1 because they have not been trained to think diagnostically about physical adaptation.
LEVEL 2: APPLIANCES AND EXTERNAL CHANGES
When technique alone is insufficient, the second line of intervention is external. Magazine loaders, slide rackers, extended controls, grip sleeves, optics upgrades, and carry reconfiguration all belong here. The majority of adaptive cases in my practice are resolved at Level 2. The gun stays stock. The shooter gains full function. I have watched students who could not load more than two rounds progress to running complete magazines within a single session after introduction of a quality loader and a grip position adjustment. That outcome required no gunsmithing. It required diagnosis.
LEVEL 3: PLATFORM AND CALIBER
If the shooter's current platform is genuinely incompatible with their physical capabilities, the third-level intervention is platform selection. A different action type, a lighter frame, a more ergonomically accessible control layout, or a reduced-recoil caliber may resolve the problem without any internal modification. Platform decisions are reversible. The shooter retains options. This level also requires the honest conversation about what the client's carry context actually demands, which may differ substantially from what they carried when the platform was originally selected.
LEVEL 4: INTERNAL MODIFICATION
Internal modification is the final resort. When Levels 1 through 3 have been genuinely exhausted and documented, it is appropriate to open the gun. A properly fitted cocking aid rather than alterations to critical geometry. Springs selected for a specific shooter and proved/tuned with their actual carry ammunition. Controls are installed because they serve the shooter's diagnosed need. Every internal change must operate within safe, professionally established parameters, must be documented in full, and must be tested to a standard that would withstand independent scrutiny.
The test standard I apply is simple and non-negotiable: if I would be uncomfortable explaining this modification to a jury and a grieving family, I do not make it. That line has kept me from a significant amount of work I was technically capable of performing. It should apply to every practitioner working at this level.
INTAKE: THE DIAGNOSTIC FOUNDATION
No adaptive intervention is legitimate without a structured intake. The intake is not a conversation about what the shooter thinks is wrong. It is a clinical observation of what the gun and the shooter reveal when they interact under no-pressure conditions. The practitioner watches, records, and forms conclusions before making a single recommendation.
| ADAPTIVE INTAKE: MINIMUM OBSERVATION STANDARDS | |
|---|---|
| Grip | Finger placement, pressure distribution, and compensatory adjustments indicating joint pain or strength deficit. |
| Slide Rack | Muscle recruitment pattern. Note failure, visible discomfort, or modified technique. Identify whether failure is strength, mobility, or technique. |
| Magazine Load | Observe unassisted loading for hand fatigue onset, dropped rounds, and pain-avoidance behavior. Record round count at failure point. |
| Presentation | Draw stroke from carry configuration. Assess smoothness, range of motion limits, tremor, and compensatory shoulder or neck movement. |
| Sighting | Whether front sight achieves usable focus. Note the head position and any accommodation indicating near-vision deficit. |
| Trigger Control | Pull weight management, flinch anticipation, and break consistency. Identify whether difficulty is strength-related or technique-related. |
| ADAPTIVE INTAKE FLOW | |||
|---|---|---|---|
| 01 OBSERVE Watch the shooter handle their firearm under no-pressure conditions. Record without interrupting. |
02 DIAGNOSE Identify whether each failure is physical, technique, or equipment-driven before recommending anything. |
03 INTERVENE Apply the lowest appropriate protocol level. One change at a time. Prove it before adding another. |
04 VALIDATE Confirm the intervention solves the presenting problem on the range with the client's actual carry ammunition. |
Every finding is documented before any recommendation is made. This documentation grounds the intervention plan in observed data rather than assumptions, and establishes the professional record that protects both practitioner and client if a modification is later questioned.
The intake also distinguishes physical limitations from technique deficits. A shooter who cannot rack the slide reliably may have a grip problem, a strength problem, or a technique problem. Each requires a different response. Installing a slide aid to address a technique problem leaves the underlying deficit unresolved, creates appliance dependency, and does not serve the shooter's long-term capability. The intake exists to prevent that error.
PROTOCOL IN PRACTICE: CASE STUDIES
The following cases illustrate the Adaptive Protocol applied in sequence. Both were resolved at Level 2. Neither gun was opened. Both clients remain active shooters.
| CASE 01 | Bilateral Arthritis, Pistol Shooter, Female, Age 71 |
| PROBLEM | Shooter could not exceed two rounds loaded before hand pain and strength failure ended the attempt. Had reduced range attendance to once monthly and had already become determined to surrender her carry permit. |
| INTAKE FINDING | Bilateral hand arthritis confirmed through observation. Significant reduction in pinch force and grip endurance. Failure point at round two of loading consistently. Grip geometry compensated toward palm rather than fingers, indicating active pain avoidance. |
| INTERVENTION | Level 1: Grip position adjusted to reduce pinch-grip reliance during loading sequence. Level 2: Quality single-round magazine loader introduced. Grip sleeve added to increase surface contact and reduce required grip force. No internal modification. Firearm remained stock. |
| OUTCOME | Load capacity increased from 2 rounds to full 10-round magazine within first session. She did not surrender the permit. She renewed it. Her words at the end of the session: I did not think I was going to be able to do this anymore. No modification to the firearm was required -- only the right diagnosis and the right tools. |
| CASE 02 | Bilateral Shoulder Impingement, Pistol Shooter, Male, Age 68 |
| PROBLEM | Shooter could not reliably cycle the slide under simulated stress conditions due to reduced shoulder range of motion and anterior deltoid weakness. Had concluded he needed to retire his carry pistol and had stopped training entirely three months prior. |
| INTAKE FINDING | Intake identified the failure point as slingshot technique requiring shoulder range of motion no longer available. Grip strength was adequate. The problem was positional, not strength-based. Current platform was otherwise appropriate. |
| INTERVENTION | Level 1: Slide racking technique revised to push-pull method using rear sight, eliminating the overhead motion driving the failure. Level 2: Extended slide release added as secondary option. No platform change. No internal modification. |
| OUTCOME | Reliable slide cycling achieved under simulated stress within one range session. He resumed training the following week and has carried consistently since. Critical finding: the problem was positional technique, not strength. A practitioner without a diagnostic framework would have sold him a new gun or sent him home. Neither was the answer. |
Not every case is resolved as easily, but this framework increases the likelihood of it happening.
LEGAL, ETHICAL, AND DOCUMENTATION STANDARDS
If you modified a carry firearm for an aging client last month and you have no documented intake, no written rationale, and no test record -- you are already exposed. Not potentially exposed...currently exposed. The modified firearm is in a holster right now. If it is used in a defensive incident, the modification will be examined. If the modification could have contributed to a malfunction or an unintended discharge, the practitioner who performed it will be accountable in a setting where reasoning and documentation are the only things standing between competence and negligence.
The defensibility standard is not a liability hedge. It is an ethical floor. A modification is defensible when it 1. improves function without compromising safety, 2. operates within manufacturer-specified or professionally established parameters, 3. has been proven with the client's actual carry ammunition to a round count that demonstrates reliability, and 4. is documented in a manner that reflects the full reasoning behind it. A modification that cannot satisfy all four criteria does not belong on a carry firearm, and perhaps any firearm.
Documentation for Level 4 work must include: the intake findings that led to the modification; the interventions considered at Levels 1 through 3 and the reasons they were insufficient; the specific modification performed and components used; the ammunition used in testing; the round count at which reliability was confirmed; and the date of completion. This record belongs in the client file and should be retained indefinitely.
The corollary obligation, and the harder one, is the ability to say no. There are presentations where the honest professional answer is that no safe modification exists that will make this firearm appropriate for this shooter at this stage of physical capability. Helping the client find a better platform, an alternative carry solution, or a different path to personal protection is not a failure of service. It is the highest expression of the professional obligation this framework establishes.
The work should disappear into the gun. The shooter should notice the function, not the modification.
WHAT HAPPENS IF THE PROFESSION DOES NOT ACT
The question is not whether the aging shooter population will need adaptive services. They already do, and the demographic curve runs in one direction. The question is whether the profession will build a framework capable of serving them or continue offering a patchwork of good intentions and inconsistent practice while the most experienced segment of the shooting population quietly exits.
The stakes are market-level as well as professional. Long-term shooters over fifty represent a disproportionate share of carry permit holders, training program enrollment, and quality firearm purchases. They are the clients most likely to refer others, most likely to invest in recurring training, and most likely to remain loyal to practitioners who genuinely solve their problems. Losing them is not a neutral outcome. It is a contraction of the highest-value segment of the customer base, driven by a professional gap that is entirely closeable.
The liability exposure is equally concrete. A gunsmith who modifies a carry firearm for an elderly client without documented intake, without a structured rationale for every decision, and without proven reliability testing is not just undeserving that client. They are carrying exposure they could not have priced into what they charge. When the modification is examined -- and in a defensive use, it will be -- the absence of documentation is not neutral. It is the record the practitioner presents to a jury.
Reputation follows practice. Shops and instructors who develop genuine adaptive competence will accumulate the referrals that come with it. Those who do not will continue losing clients at the stage when those clients need the most support and are most likely to tell others what they found. Within five years, adaptive intake and documentation will separate professional shops from hobby-level work. The practitioners who move first own the standard.
Beyond the business argument is a simpler one. These are people who have spent decades taking personal protection seriously. They have trained, carried, and built skills that represent real investment in their own safety and the safety of people they love. They deserve a professional framework that matches that investment -- not a quiet suggestion that they find another hobby.
Adaptive Gunsmithing is presented here as a distinct professional discipline with its own intake standards, intervention hierarchy, documentation requirements, and ethical floor. It is not a refinement of existing practice. It is a new category of professional obligation, and it belongs in every serious instructor's methodology and every working gunsmith's service offering.
WHAT DEFINES AN ADAPTIVE-CAPABLE SHOP
The minimum professional standard. Not a certification. A benchmark.
01 Structured intake performed on every adaptive client before any recommendation is made.
02 All intake findings documented in the client file prior to intervention.
03 Protocol level documented for each intervention with rationale for advancing to the next.
04 Level 4 modifications tested with client's actual carry ammunition to a confirmed round count.
05 Client files retained indefinitely and available for professional review.
06 Every recommendation defensible in plain language to a non-specialist audience.
A shop that meets these standards is not doing more than others. It is doing what the work has always required.
The future of the profession will not be defined by who builds the best gun.
It will be defined by who keeps the most people capable of using one.